Years ago, while studying to be a paramedic, I learned about the 7 Stages of Death and Dying, first described by psychiatrist Elizabeth Kubler-Ross. Over the decades since, I have watched those same stages play out in disaster after disaster — not just in survivors picking through the wreckage of their homes, but in the responders standing next to them. We all process catastrophic loss differently. I have been unfortunate enough to witness it far too many times, from both sides of the line.
When disaster strikes — a wildfire, flood, tornado, earthquake, or any sudden event that strips away what felt permanent — the visible losses are immediate. The home, the neighborhood, the routine, the sense of safety. What is less visible, and far less talked about, is the grief that follows. Not necessarily grief for a person, but grief for what was. That grief is real, it is recognized by mental health science, and it follows a predictable path.
That predictability matters. When you know what is coming, you can name it. When you can name it, you can manage it. And when you can manage it, you make better decisions at exactly the moment when decision quality determines everything — whether your insurance claim survives, whether your family holds together, whether you rebuild or give up.
This is not a clinical document. It is what thirty years of watching people go through the worst days of their lives has taught me, layered on top of what the science says. Read it now, before you need it. Or share it with someone who already does.
“Most people in the first 72 hours after a disaster believe they are handling it well. They are not. Acute stress impairs judgment, working memory, and risk assessment in ways the person experiencing it cannot detect from the inside.”
The Population Arc: What Communities Experience
Before looking at individual grief, it helps to understand the broader trajectory that disaster-affected communities follow. This timeline, documented by disaster mental health researchers and embedded in how SAMHSA and the Red Cross train responders, maps the emotional arc at the community level. Your individual experience may not follow it exactly — but understanding where the population tends to be helps explain the environment you are navigating.
Shock, dissociation, hypervigilance, sleep disruption, appetite loss, irritability. Most consequential decisions get made here. Impaired judgment is at its peak. Most people do not recognize these as trauma responses — they believe they are “handling it well.”
Community solidarity is high. Adrenaline is still elevated. There is a palpable “we got this” energy. This phase looks healthy and often is. It is also frequently masking an accumulating trauma debt that will surface later. People defer their own care to help others.
The bottom drops out. Insurance denials hit. Contractors are unreliable. Aid moves slower than expected. Substance use spikes. Domestic violence spikes. Suicide ideation spikes. This is statistically the deadliest phase psychologically — and exactly when external support has faded and media attention has moved on.
Rebuilding meaning, integrating the loss. Post-traumatic growth for some; chronic PTSD for others. Predictable anniversary reactions for years. The trajectory from here depends heavily on whether support was available during Phase 3.
Notice the gap: community support, media coverage, and volunteer resources tend to peak during Phase 2 — and then collapse. The people who need the most help in Phase 3 are navigating it largely alone. If you are reading this in Phase 3, that is not a coincidence. That is the design flaw in how we as a society respond to disaster. Name it. It is not a personal failing.
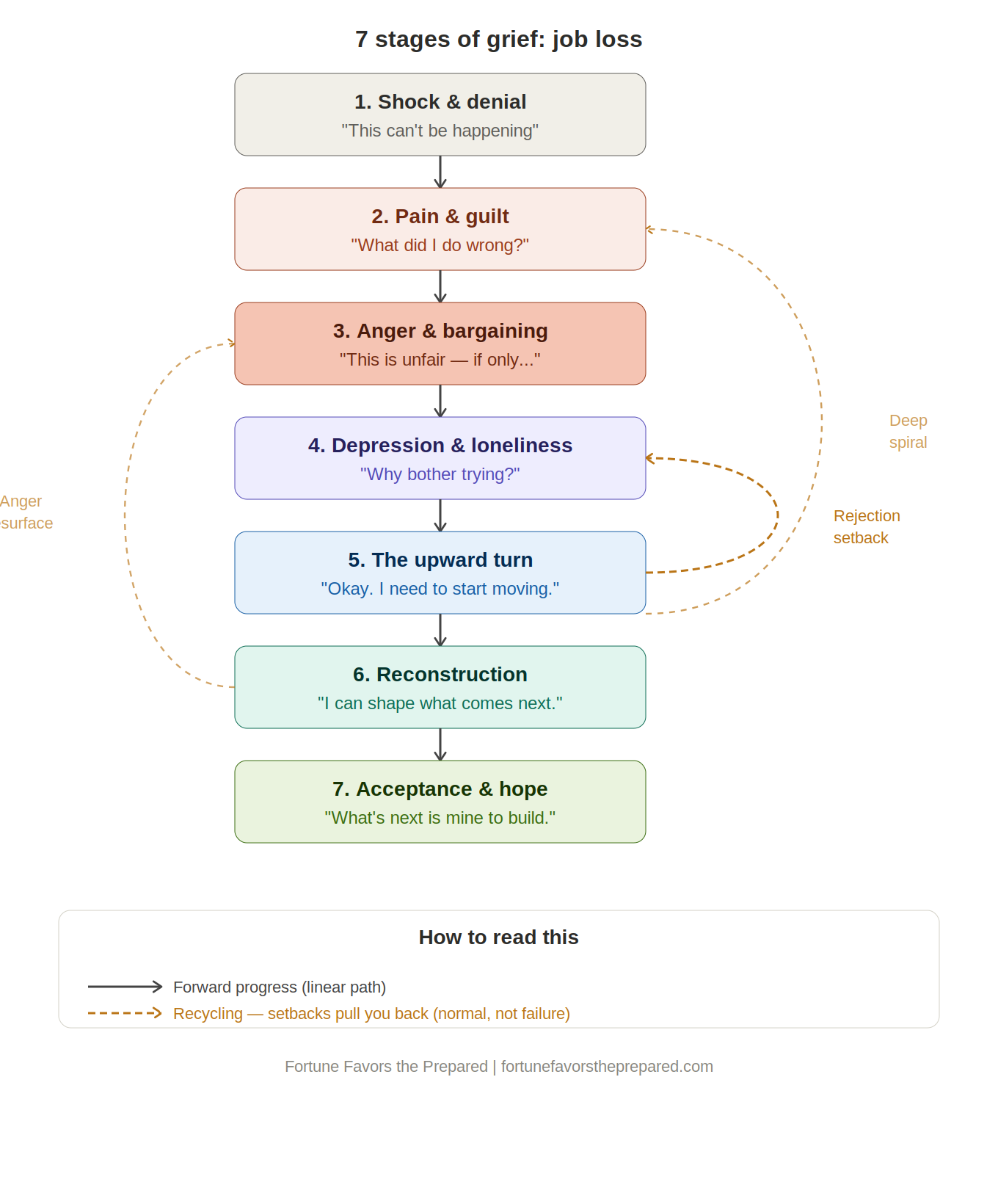
The 7 Stages of Grief, Applied to Disaster Loss
Kubler-Ross originally developed her framework for people facing terminal illness and death. What she documented — and what has been observed in disaster settings ever since — is that profound loss, of any kind, tends to move through recognizable emotional territory. The loss does not have to be of a person. The loss of a home, a neighborhood, a way of life, a sense of safety — these trigger the same grief response.
These stages are not steps on a checklist. They are territories. You may spend weeks in one, hours in another. You may skip one entirely and then find it waiting for you six months later. The map is not the territory — but having a map still helps.
Shock and Denial
In the first hours and days after a disaster, the mind protects itself with numbness. You may feel strangely calm, almost detached from what is happening around you. Some people describe watching themselves move through the immediate aftermath as if observing from a distance. You may find yourself minimizing the damage, certain that things will somehow return to normal quickly, making plans based on an optimistic assessment that does not match reality.
This is not weakness. It is a neurological protection mechanism. The brain manages an unbearable information load by throttling it. Shock is adaptive in the short term — it allows you to function when full emotional processing would be incapacitating. The problem is that shock impairs judgment in ways that are not visible to the person experiencing it.
This is why the single most important rule of early disaster recovery is: do not make irreversible decisions in the first 72 hours. Do not sign contractor agreements. Do not accept insurance settlements. Do not agree to anything permanent. The person making those decisions is not operating at full capacity, no matter how certain they feel.
The workbook that gets you ready for the year after.
The single most important rule of Stage 1 is: don’t make irreversible decisions in the first 72 hours. But knowing that rule doesn’t help if you don’t already know your insurance policy, your FEMA IA deadlines, or what receipts to keep. The Household Recovery Workbook is designed to be completed before a disaster — so that when shock hits, the answers are already written down.
Pain and Guilt
As the protective numbness of shock begins to recede, pain rushes in to fill the space. Not just grief for what was lost, but something sharper: the conviction that the loss was preventable, and that you are responsible for not preventing it. Survivors of disaster replay decisions with exhausting intensity. The evacuation they delayed by a day. The documents they didn’t put in a waterproof bag. The neighbor they meant to check on. The emergency kit they always intended to build.
Responders are not immune. First responders, emergency managers, and volunteers who worked the event often carry a parallel guilt: the call they couldn’t get to in time, the resource that wasn’t available, the person they couldn’t reach. The operational debrief and the emotional debrief are separate processes, and both matter.
Here is what the guilt rarely accounts for: disasters are low-probability, high-consequence events specifically designed by their nature to outpace normal human preparation. The person who didn’t evacuate early enough was probably weighing real competing considerations — work, family, previous false alarms, uncertainty about the threat level. The family without a 72-hour kit was not uniquely irresponsible. Most households are not prepared. That is a systemic failure, not a personal one.
That does not make the guilt disappear. But naming it for what it is — a normal grief response, not an accurate indictment — creates enough space to keep functioning.
Anger and Bargaining
Grief turns outward. The anger that arrives in Stage 3 is often indiscriminate — directed at government agencies, emergency management systems, neighbors who seemed to fare better, insurance companies, contractors who overpromise, aid organizations with confusing eligibility requirements. The anger is real, and often some portion of it is justified. Systems do fail. Warning times are sometimes inadequate. Insurance companies do behave badly. These are legitimate grievances.
What makes this phase dangerous is that anger degrades decision quality in specific ways. It increases risk tolerance. It creates urgency that doesn’t match the actual timeline of recovery. It makes people sign agreements they shouldn’t sign, make accusations that complicate later negotiations, and burn relationships they will need in the months ahead. The contractor who shows up on Day 3 offering to start work immediately, cash up front — he is counting on Stage 3 grief to close the deal.
Bargaining runs alongside the anger: “If FEMA approves the claim, everything will be okay.” “If we can just get back into the house by [date], we can manage.” These conditional frames create false finish lines that, when they move — as they almost always do — produce a secondary collapse. Recovery timelines for significant property damage are measured in months to years, not weeks. That is not pessimism. It is operational reality, and building against it protects you from unnecessary secondary grief.
Depression and Loneliness
This is the heaviest stage, and statistically the most dangerous. The adrenaline that sustained the acute phase is gone. The community solidarity of the first weeks has faded. The volunteers have gone home. The media coverage has moved to the next event. Your support network, having rallied in the first weeks, has returned to the demands of their own lives. And you are still in the middle of it.
This is the disillusionment phase at the individual level. Insurance denials hit. The adjuster’s assessment comes in lower than expected. A contractor disappears after taking a deposit. FEMA assistance is less than you needed. Temporary housing is cramped and disorienting. The children are struggling in new schools. The workplace is losing patience. And the timeline to resolution keeps moving.
The behavioral signs of this stage — withdrawal from social contact, substance use, neglect of self-care, increased family conflict, inability to manage the practical work of recovery — are not character failings. They are predictable physiological and psychological responses to sustained, compounded loss under conditions of inadequate support. Knowing that does not make them easier. But it does mean that professional support is appropriate, effective, and warranted — not as a last resort, but as a reasonable response to an unreasonable situation.
The people most at risk in this phase are often the ones who appeared to be managing best in the early stages. Caregiver burnout is real: the person who held the household together through the acute phase may be the one who crashes hardest when the scaffolding comes down.
The Upward Turn
At some point — and the timing varies enormously from person to person — the weight lifts slightly. Not gone. Not resolved. But manageable in a way it wasn’t before. Energy returns in fragments. The paralysis that made simple decisions feel impossible begins to ease. You make a call you’d been putting off, and it goes better than expected. You attend a recovery meeting and feel, for the first time, that the people running the process might actually be competent.
This phase can be fragile. A denial letter, an unexpected repair cost, a contractor setback, or an anniversary date can temporarily push someone back into depression or anger. That is not regression. That is the normal, nonlinear shape of grief. The stage model is a map, not a railroad. Most people cycle through earlier stages multiple times before the upward turn becomes more durable.
What characterizes this phase is not optimism — it is not that everything feels okay, or that the losses feel smaller. It is that action becomes possible again. The gap between knowing what needs to be done and being able to do it begins to close. That is enough. Start there.
Reconstruction
Reconstruction is the work phase — not just of the physical structure, but of life. Active decision-making replaces reactive crisis management. Strategic thinking about the future becomes possible. You are not just responding to what the disaster did; you are making intentional choices about what comes next.
The emotional processing that was impossible in earlier phases becomes accessible now. People in this phase often find themselves able to think clearly about what the loss meant, what they want to preserve from the life they had, and what they might choose to change. Some of the most important decisions of a person’s life get made in this phase — about where to live, what to prioritize, what kind of community to invest in. Making those decisions consciously, with adequate information and support, produces better outcomes than making them reactively.
Reconstruction is also where the practical work intensifies: contractor management, insurance negotiations, FEMA appeals, financial planning for the long rebuild. Having documented everything in the acute phase pays dividends here. The household with a complete paper trail wins disputes that the household without one loses.
Acceptance and Integration
Acceptance is not erasure. It does not mean the loss was acceptable, that the damage was fine, or that things are back to the way they were. They are not. Recovery restores function; it does not restore the original. The house may be rebuilt, but it is not the same house. The neighborhood may recover, but some neighbors did not come back. The sense of safety may return, but it carries a different texture — one that knows, now, what can happen.
What acceptance does mean is that the event has been integrated into the story of who you are, rather than remaining an open wound that defines everything. The grief is there, but it is not consuming. You can think about what happened without being pulled under. You can talk about it, plan against recurrence, even help others navigating the same territory.
For some people, this phase brings what researchers call post-traumatic growth: a reprioritization of what matters, a deeper connection to community, a clarity about values that crisis strips down to the essential. For others, this phase requires ongoing professional support and never fully resembles what came before. Both outcomes are real. Both are valid. The measure is not how fully you’ve “recovered” — it is whether you are moving through it, with support, toward a life that functions.
What Your Body and Mind Will Tell You
Trauma responses span four categories. Knowing what is normal versus what needs professional intervention helps you respond appropriately — and helps you advocate for the people around you who may not recognize their own symptoms.
Most of these responses are normal for the first four to six weeks after a disaster. They become clinically concerning when they intensify rather than ease over time, when they substantially impair daily functioning, or when the high-risk indicators in Part V emerge.
Physical
- Sleep disruption (insomnia, nightmares, broken sleep)
- Appetite changes (loss or comfort eating)
- Hypervigilance, exaggerated startle response
- Headaches, GI distress, muscle tension
- Persistent fatigue not relieved by rest
- Increased susceptibility to illness
Cognitive
- Intrusive memories or flashbacks
- Difficulty concentrating, forgetfulness
- Decision paralysis on complex tradeoffs
- Impaired risk assessment (especially financial)
- Confusion about time and sequence of events
- Catastrophic thinking patterns
Emotional
- Numbness, emotional flatness
- Irritability, short fuse
- Guilt (survivor’s guilt, decision guilt)
- Shame about accepting help
- Hopelessness, especially in disillusionment phase
- Sudden, unexpected grief episodes
Behavioral
- Withdrawal from social contact
- Substance use (alcohol especially common)
- Increased family conflict
- Neglect of self-care, hygiene, medication
- Avoidance of anything associated with the event
- Loss of interest in previously enjoyed activities
Your Household: Children, Elders, and the Caregiver
Disaster affects every member of a household, but not in the same way or on the same timeline. A household that manages the recovery well does so by accounting for every member’s specific needs — not just the adults managing the logistics.
Children, by age
Children cannot articulate what they are experiencing in the way adults can. Their grief manifests behaviorally, and what looks like defiance or regression is often a trauma response. Knowing what is normal for each age group helps you respond appropriately rather than reactively.
- Increased clinginess, separation anxiety
- Sleep regression, feeding changes
- Increased crying, harder to soothe
- Loss of recently acquired skills
- Regression to younger behaviors
- Repetitive play re-enacting the event
- Unusual new fears or phobias
- Increased clinginess or withdrawal
- Difficulty concentrating, academic decline
- Withdrawal from previously enjoyed activities
- Physical complaints (stomachaches, headaches)
- Aggression, irritability, sleep disturbance
- Withdrawal, isolation, increased screen use
- Risk-taking behaviors
- Substance experimentation
- Academic decline, increased family conflict
Older adults
Elders are frequently the most underserved population in disaster recovery, because they self-isolate and do not ask for help. Cognitive symptoms in this group may resemble dementia onset — they are often trauma responses. Physical complaints frequently mask emotional distress. Medication non-compliance during stress is common and dangerous. Daily check-ins, in person if possible, are the single most useful intervention. Help with the cognitive load of recovery logistics — insurance calls, FEMA registration, contractor scheduling — may exceed current capacity even in people who were previously highly capable.
The caregiver
Every household has someone who functions as the primary organizer of the recovery. That person is at high risk of caregiver burnout — a syndrome that looks like exhaustion that doesn’t lift, increasing irritability, neglect of their own health, resentment, and loss of meaning. The spouse who appears to be managing everything competently is often the person closest to collapse. Caregiver burnout needs to be actively watched for and built against — not as a nice-to-have, but as a recovery planning item.
Psychological First Aid: How to Help the People Around You
Psychological First Aid (PFA) is a specific protocol developed for non-clinicians — household members, neighbors, coworkers, community members — to support people in acute distress. It has a strong evidence base and is taught by SAMHSA, the Red Cross, and the National Child Traumatic Stress Network. You do not need clinical training to use it.
The core of PFA is not advice-giving. It is presence, safety, and listening. The single most useful skill is showing up and staying — not solving, not fixing, not advising. Most people in acute distress need to be heard before they need any of those things. Sit with them. Let silence be acceptable. Let them lead.
What helps
- I’m here. You’re not alone in this.
- What do you need most right now?
- This is hard. What you’re feeling makes sense.
- I’m not going anywhere.
- Take your time.
- Would it help if I [specific concrete offer]?
What doesn’t help
- “I know how you feel.” (You don’t.)
- “At least…” (Any sentence starting this way minimizes.)
- “Everything happens for a reason.”
- “You’re so strong.” (Pressures performance.)
- “You should…” (Unsolicited advice rarely helps.)
- “It could be worse.” (Comparative suffering doesn’t console.)
Plan for the predictable difficult dates: one month, six months, one year, and multi-year anniversaries of the event. These consistently produce emotional setbacks even in people who have reached acceptance. Consider scheduling therapy appointments around these dates. Notify your support network in advance. Anchor the date with something intentional. The people who navigate anniversaries best are the ones who planned for them rather than being ambushed.
These stages are not linear. Most people cycle through them repeatedly — reaching what feels like acceptance, then getting hit by a bureaucratic setback, a contractor problem, a family conflict, or an anniversary date that pulls them back into anger or depression. That is not regression. That is the normal, nonlinear shape of grief after disaster.
The goal is not to complete the stages in sequence and arrive at acceptance permanently. The goal is to keep moving through them, with adequate support, in a direction that allows life to function. Some days that means progress. Some days it means staying in place. Both count.
If you are reading this and recognizing yourself or someone you love in the harder stages — that recognition is itself a form of progress. You cannot navigate terrain you cannot see.
When to Call for Help Now
Some symptoms require immediate professional intervention rather than peer support or self-management. If you observe any of the following in yourself or someone in your household, act immediately:
- Any expression of suicidal ideation, even casual ones (“I just want it all to end”)
- Substance use spike well beyond previous baseline
- Dissociation lasting hours — not present, not responsive, unreachable
- Domestic violence onset or escalation
- Children showing dangerous behavioral changes (self-harm, refusal to eat, complete withdrawal)
- Inability to perform basic self-care for several consecutive days
- Psychotic symptoms: hallucinations, delusions, paranoia not present before
Be direct with the person you are concerned about: “I’ve noticed [specific changes]. I’m worried about you. Are you okay?” Listen without judgment. Do not promise to keep secrets if safety is at stake. Offer to call together. If they refuse and you remain concerned, call SAMHSA or 988 yourself for guidance.
Crisis resources — available 24/7
The operational playbook for the year after disaster.
Everything in this article — the phase timeline, the mental health stages, the household and children’s sections, the PFA protocol, the crisis escalation guide — goes deeper in the Household Recovery Workbook. Plus the practical work that grief won’t do for you: insurance claims, FEMA IA applications, contractor vetting, vital records recovery, and the tax implications nobody tells you about.
When shock hits, you will not research your insurance policy. You will not look up FEMA deadlines. You will not know which receipts to keep or when the SBA disaster loan window closes. Section 1 of this workbook is designed to be filled out now, while you can think clearly — so that the answers exist when your judgment is impaired and the clock is running. The household that walks into the recovery process with a completed workbook wins disputes that unprepared households lose.
- 168 pages, loose-leaf, binder-ready
- Pre-fill section to complete before disaster
- Insurance, FEMA IA, SBA, contractor, tax, and mental health sections
- Worksheets, checklists, decision frameworks, and reference tables
- Part V: Mental health phases, PFA, children, elders, caregiver burnout
- Family Emergency Plan Workbook + Household Recovery Workbook
- Plan the response before the disaster
- Recover from it after
- Two workbooks, one bundle
- Family Emergency Plan Workbook
- Personal Preparedness Assessment Workbook
- Household Recovery Workbook
- Next of Kin Workbook
Patreon supporters at the $11.95 tier or above receive member pricing on all workbooks. Already own the Family Emergency Plan Workbook? Your discount code is on the inside cover.